Imaging of the trachea and main stem bronchi is an essential preliminary step to endoscopic resection in patients with malignant tracheobronchial disease or tracheal stenosis. However, patients may present quite dyspneic and require immediate intervention which can often preclude a thorough radiological work-up prior to the procedure. Whenever possible, available imaging studies should be correlated with endoscopic findings. Radiographic studies are also essential in evaluating the outcome of a procedure, ruling out immediate complications, and in providing long-term follow-up.
 The standard battery of tests ordered in our patients is generally the following :
The standard battery of tests ordered in our patients is generally the following :
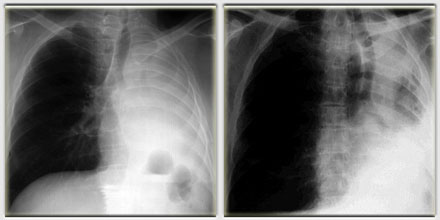
 Chest radiographs (PA and lateral views). Initial x rays provide essential information regarding the size, location, and impact of a given lesion on a patient’s respiratory status. The quality of these studies should be optimized as they may be the only document available to the endoscopist prior to the procedure.
Chest radiographs (PA and lateral views). Initial x rays provide essential information regarding the size, location, and impact of a given lesion on a patient’s respiratory status. The quality of these studies should be optimized as they may be the only document available to the endoscopist prior to the procedure.
Special studies focusing on the cervical region or the mediastinum may provide clues as to the degree of tracheo-bronchial involvement by disease.
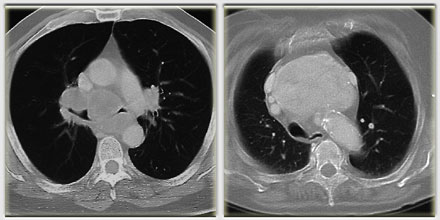 Even though chest radiographs alone may suffice in order to establish with some precision the degree of tracheo-bronchial involvement, computer assisted tomography (CAT) scans are recommended in most cases if the patient’s condition will allow it. CAT scans can help clarify anatomical relations within the area of interest, in particular the potential involvement of major mediastinal vessels by disease.
Even though chest radiographs alone may suffice in order to establish with some precision the degree of tracheo-bronchial involvement, computer assisted tomography (CAT) scans are recommended in most cases if the patient’s condition will allow it. CAT scans can help clarify anatomical relations within the area of interest, in particular the potential involvement of major mediastinal vessels by disease.
Vascular studies in general are not routinely ordered, but if vascular involvement is suspected, they can be quite useful. Bronchial arteriography can determine the vascularity of a given tumor, while angiograms of the superior vena cava or the pulmonary arteries are sometimes ordered in order to investigate potential tumor invasion of these structures.
 Either tracheography or bronchography are contraindicated in severe obstruction of the central airways. Contrast material can be very dangerous in patients scheduled for endoscopic resection. In particular, viscous products can complicate tight stenoses leading to complete obstruction of the airway and precipitate respiratory distress in these fragile patients. On the other hand, bronchography can be useful in assessing the evolution of chronic endobronchial obstruction by a slow growing tumor, following endoscopic resection.
Either tracheography or bronchography are contraindicated in severe obstruction of the central airways. Contrast material can be very dangerous in patients scheduled for endoscopic resection. In particular, viscous products can complicate tight stenoses leading to complete obstruction of the airway and precipitate respiratory distress in these fragile patients. On the other hand, bronchography can be useful in assessing the evolution of chronic endobronchial obstruction by a slow growing tumor, following endoscopic resection.
The radiographic evaluation of most patients undergoing laser resection rarely has diagnostic value because most patients have been carefully studied before being referred to us for endoscopic intervention. The role of the radiological work-up is none the less essential to the endoscopist in planning a safe resection.
Critical information provided by imaging studies includes :
The pulmonary status of the patient. The images provide information regarding lobar ventilation, retention of secretions, the presence of emphysema or a trans-mediastinal hernia.
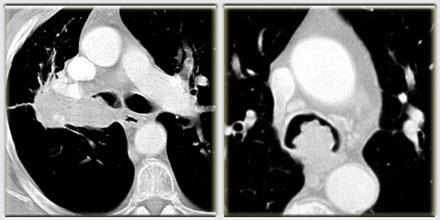
The severity of the obstruction. Standard radiographs may localize the lesion and determine its relationship to major landmarks such as the vocal cords, carina, and main stem bronchi. The CAT scan provides greater detail at the level of the main stem and peripheral bronchi. It is possible to appreciate tumor extension, the severity of the obstruction and its anatomical repercussions, in particular with respect to the tracheo-bronchial axis.

Tumor invasion. Extrabronchial extension should be sought in order to prepare for potential complications during resection. Para-tracheal or bronchial wall involvement may be assessed based on wall thickness as seen on imaging studies. Esophageal involvement, however, is often difficult to assess. CAT scans are very useful in determining tumor invasion of mediastinal structures.

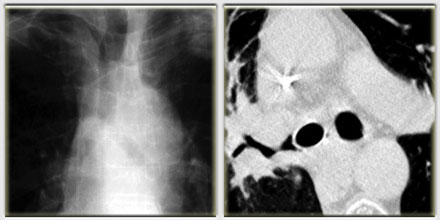
The anatomical context. That is, the localization of the tumor with respect to major anatomical landmarks such as the main vessels of the mediastinum, aorta, brachycephalic plexus, pulmonary artery etc…
Associated pathology. Imaging studies may help in the detection of tracheo-esophageal fistulas. Sometimes it is best to plan esophagoscopy prior to endoscopic resection.
 Post-operative imaging studies can be obtained under more favorable circumstances, once the immediate danger of impending respiratory failure has been averted by endoscopic resection. Special studies can be ordered to evaluate the immediate outcome of the procedure (resolution of atelectasis, airway patency, impact on the lung parenchyma distal to the obstruction), but also as a means of long-term follow-up.
Post-operative imaging studies can be obtained under more favorable circumstances, once the immediate danger of impending respiratory failure has been averted by endoscopic resection. Special studies can be ordered to evaluate the immediate outcome of the procedure (resolution of atelectasis, airway patency, impact on the lung parenchyma distal to the obstruction), but also as a means of long-term follow-up.


