|
|
 |

Index >
Technique > Intubation |
Intubation |
|
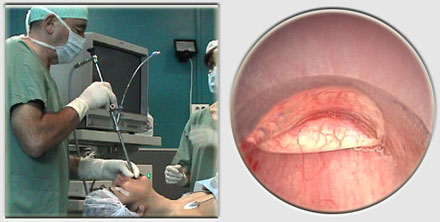
Successful rigid bronchoscopic intubation requires a great deal of experience. The safest method is the classical approach using the telescope to view the tip of the bronchoscope and the airway distal to it.
The patient is supine and the neck hyperextended. The upper teeth are protected by the left thumb, which must support the entire pressure of the rigid tube. The teeth should never be used as a fulcrum. Care should be taken to avoid damage to the lips which can be caught in between the bronchoscope and the teeth during intubation. The beveled tip of the bronchoscope should always be anterior. This film illustrates the appropriate progression in rigid bronchoscopic intubation of the trachea, including protection of the upper gums and teeth with the left thumb, positioning of the bronchoscope, and subsequent steps to follow.
The mouthguard can be a simple gauze or a specially designed plastic mouthpiece. Following intubation an ambu bag is coupled to the bronchoscope’s side-port facilitating oxygenation of the patient as needed. A closed circuit can also be established if desired.
|




|
move
up
|
move
down
|
|
previous
|
next |
