|
|
 |

Index > F.A.Q. |
F.A.Q. |
|
Question : Why do you prefer to use a rigid bronchoscope for therapeutic endoscopy ? Answer by Jean-François Dumon, M.D. The open tube is the instrument of choice for most resection procedures. This is because its working channel is large enough for viewing, suctioning, and lasing at the same time. This is a great advantage particularly in case of flooding of the airways by blood, secretions and/or pus. Another non-negligible advantage is the possibility to make mechanical debridment with tip of the bronchoscope and insert stents. Since the introduction of the fiberscope, the rigid bronchoscope has been used less. In fact, many younger endoscopists have only limited experience with it. This state give many the impression that the fiberscope rendered the open tube obsolete.Unfortunately training in the use of the rigid open tube system has been all too often neglected. Though it is unusual, massive hemorrhages can also occur during diagnostic bronchoscopy so that even diagnostic endoscopists should know how to use a rigid open tube and have one on hand to handle this possibility. Question : The main problem is to find a place to learn the technique of rigid endoscopy. Where can I learn this technique ? Answer by Jean-François Dumon, M.D. There are many places specialized in therapeutic endoscopy, do not hesitate to spend some time with skilled endoscopists.
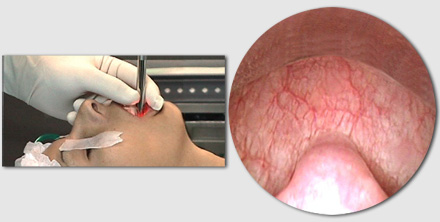
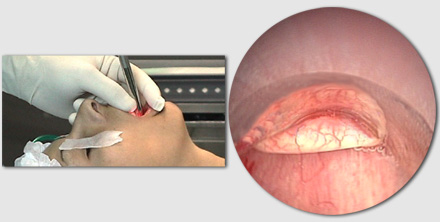
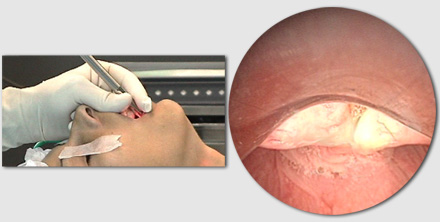
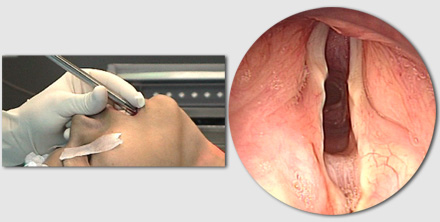
Rigid endoscopy is not dangerous if you understand that you have to adapt the anatomy to your instrument. Precautions start at the insertion : Insertion of a rigid open tube bronchoscope requires training. The safest method is insertion under direct visual control through the illuminated telescope which should not overextend the end of the rigid open tube in order to avoid soiling. The patient is in the supine position with his head in hyperextension. The upper teeth are protected by the index finger of the left hand (for a right-handed endoscopist). The teeth must never be used as a fulcrum. Care must also be taken not to pinch the upper lip between the teeth and the bronchoscope. The first land mark is the uvula By tilting the bronchoscope upwards, the barrel of the tube follows the base of the tongue and is brought to bear against the epiglotis which is thus lift up. The key landmarks in insertion are the arythenoids. The vocal cords By rotating the bronchoscope one fourth turn, the beveled tip of the tube can be used to carefully push one vocal cord aside and the trachea can be entered. After the insertion the most important thig is to adapt the anatomy of your patient to the bronchoscope. This can be done only by moving the position of the head. The bronchoscope always should be in the axis of the trachea or the bronchi. Question : Do we always have to extubate and re-intubate a patient every time we change a tube - isn’t there a method to avoid this ? Answer by Jean-François Dumon, M.D. There is an interesting technique which consists of first intubating the patient with a short, large diameter tracheal tube. An intermediary connector fitted with a silicone cap is then connected to this tube, allowing longer bronchial tubes to be passed through it. This approach is possible with the bronchoscope EFER-DUMON® because its design has no light carrier and is perfectly cylindrical, which is not the case with most bronchoscopes whose tubes are oval-shaped. Question : What are the main indications for therapeutic endoscopy ? Answer by Hervé Dutau, M.D. The main indications for therapeutic bronchoscopy are :
Question : When do you think that there is an indication for stenting the airway ? Answer by Hervé Dutau, M.D. There is an indication for stenting the airway in case of :
|
|
move
up
  move
down move
down |
